


It was midnight, about 12 hours into her visit to the emergency department at the QEII, and still 24-year-old Ariel McTavish hadn’t seen a doctor. She had contemplated leaving; the wait wasn’t just long, it was terribly uncomfortable. She was cold, wearing just a johnny shirt. She was vomiting into a bag. She was there alone. “I don’t like to make a fuss and drag someone with me,” she says.
The ER was crowded, so at one point she shared a room with another patient—an older man, intoxicated and shouting profanities. She waited there for more than an hour before a nurse noticed her discomfort and moved her to an exam room across the ER bay.
She wanted to leave, but her condition had worsened. She felt a familiar and overwhelming pain radiating like a fire through her body: A cyst on her ovary had ruptured.

McTavish, who has endometriosis, knows the excruciating pain of a ruptured ovarian cyst. This was in 2017, and it was the sixth time she’d suffered one.
A ruptured cyst is typically managed by treating the pain with medication through an IV, and watching it closely by ultrasound. In some cases, ruptured cysts lead to internal bleeding or require emergency surgery.
But the on-call doctor, when he came to examine McTavish at 2am, wasn’t thinking about emergency surgery. Patients with ruptured ovarian cysts typically have a fever, and she didn’t. This was normal for McTavish—all but one of her ruptures happened without a fever. Still, the doctor told her he wouldn’t send her for an ultrasound, despite her other symptoms: extreme pain, bleeding, vomiting.
He asked if she was experiencing period pains, then told her she should go home. She refused.
“I wasn’t leaving. I had waited 14 hours, throwing up into a bag, I was put in a room with an angry drunk man while nearly naked and left unattended,” McTavish says. “I’m obviously suffering or I wouldn’t have left myself in that situation.”
The doctor didn’t seem to believe her.
“I remember his exact words to me: ‘You know this looks like drug-seeking.’”
She left without an ultrasound.
The gap in uterine care
Endometriosis, which affects one in 10 Canadians with uteruses, is the often misunderstood condition when tissue that normally lines the uterus grows in other parts of the body. The misplaced tissue is best known for causing chronic pain, cysts, internal scarring and fertility issues. It’s most commonly found in ovaries, fallopian tubes and pelvic tissue, but can be elsewhere in the body. The best treatment, alongside pain and hormone medications, is surgical—a laparoscopic incision to carefully cut out endometriosis tissue. This surgery improves the condition, but it’s not necessarily a cure, because the tissue can grow back.
The worst part of living with endometriosis is trying to convince people the pain is real, now-30-year-old McTavish says. Weeks after this emergency visit, an ultrasound ordered by her family doctor confirmed an ovarian cyst had ruptured.
Knowing she was right brought her little comfort. “I just got lucky it wasn’t a more serious cyst,” she says.
“Most times, talking about endometriosis to medical professionals here feels like you’re screaming and no one is listening.” It felt this way, too, in the 20 months McTavish waited with chronic pain and no answers before a specialist was available to diagnose her via laparoscopic surgery in 2015.

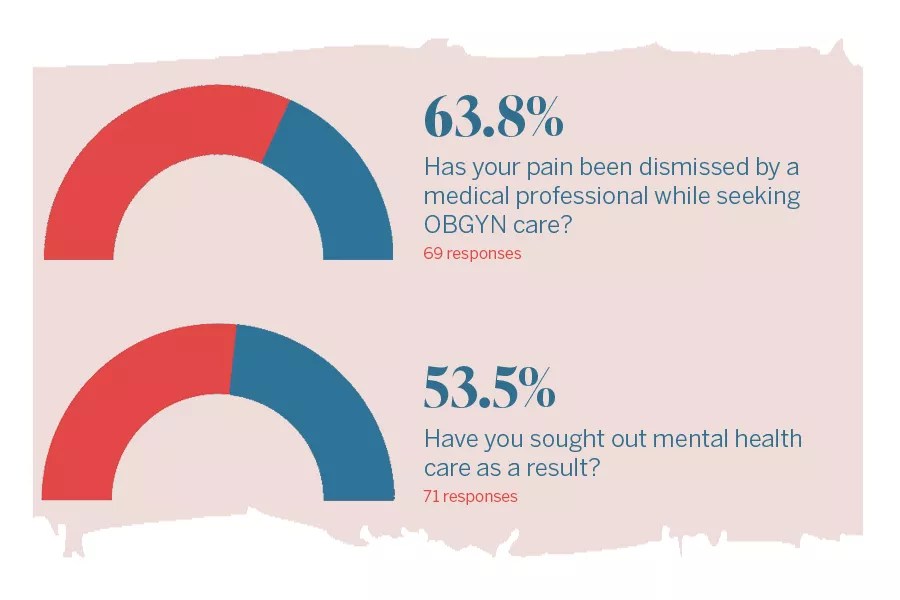
Stories like McTavish’s are far too common in Haligonians seeking gynecological care. More than 70 people completed a survey from The Coast collecting detailed information about seeking OBGYN care while living in Halifax (we made the survey after a callout for potential interview subjects got more attention than expected). Of those who shared their stories in the survey, 64 percent say their pain was dismissed by a medical professional while seeking care.
“I never know how I will be treated by any health care professional and whether they will take me seriously or not. Most times it feels like I have exhausted all treatment options and am wasting everyone’s time,” one respondent says. “It feels very hopeless.”
Doctors may have a tendency to brush off women’s pain. This is worse for patients who are not white; numerous studies report implicit racial biases present in medicine—including a 2019 report that found Black patients are less likely to be treated for acute pain. Women of colour, particularly Black women, are less likely to have their health concerns taken seriously.
The surveyed individuals sought out care for a number of reasons. The vast majority were looking for answers related to painful symptoms that could be tied to conditions like endometriosis or polycystic ovarian syndrome. Some sought out surgical birth control, others had trouble getting pregnant.
Serious gynecological conditions, including cervical cancer, are on the minds of some survey respondents. Four respondents say they are worrying about cancer as they await biopsies or other tests. One woman, who had a biopsy to examine endometrial abnormalities while living in Manitoba, has been waiting two years for a second biopsy to be done in Nova Scotia.
“What if these abnormalities have developed into cancer? I wouldn’t know, because I don’t have the care I should here in Nova Scotia,” she says.
The survey participants—a group of women, non-binary people and trans men living in Halifax Regional Municipality, aged 22 to 46—shared their varied experiences navigating the gynecological health systems. Their experiences vary widely, but many concerns were repeated. The words “debilitating,” “hopeless,” “gaslit” and “excruciating” appear repeatedly.
“I started questioning my own sanity. I constantly had doctors telling me my pain didn’t exist,” says one respondent.
“I feel like I have nowhere else to turn. In Canada, we have to take what we can get and if the doctor doesn’t believe you, that’s often the end of your care,” another says. “It is beyond frustrating.”
Long waits for help
The average wait time for an OBGYN among the respondents was 14 months, with some waiting as long as three and a half years. More than 20 people, 28 percent, are still waiting to hear from a specialist.
“When I finally did find a doctor who took me seriously, he was horrified that it had taken so long for me to get care,” one respondent says.
“The wait lists are way too long,” says another.
Nova Scotians looking to see an OBGYN for any number of non-urgent concerns, including chronic uterine issues and painful endometriosis symptoms, will wait 12-18 months to see a specialist. Compare this to Ontario, where non-urgent gyno referrals take less than three months, according to a 2018 study.

The delays in Nova Scotia have worsened during the COVID-19 pandemic: the province’s gynecological waitlists are 29 percent longer than they were before COVID. This is largely due to paused services during earlier waves of the pandemic, says a spokesperson for the IWK Health Centre.
“Having to wait for years to see an OBGYN for a debilitating problem isn’t right,” one woman says.
“I have not received even a rough date or an idea of when my appointment could be. I am in pain that affects my everyday life, my work and especially my education,” says another survey respondent.
“Being brushed off, again and again, is crazy-making. I have been reporting daily pain and irregular bleeding for almost a year,” one respondent says. “I feel like my pain doesn’t matter and won’t matter until I pass out or die.”
The province has made steps in supporting those with endometriosis and chronic pelvic pain by establishing a specialized clinic at the IWK, where patients can be seen by a gynecologist, physiotherapist, social workers, nurses and a nurse practitioner. The pilot enrolled 12 patients, though they didn’t all complete the three-month program. It restarted in January with another 12 patients.
Leah Pink, a nurse practitioner who works at the specialized clinic, says it’s an ideal setting for combining multidisciplinary approaches to treating endometriosis in those who didn’t respond to first- or second-line treatments (including laparoscopy and hormones). She’d like to see the program expand.
“Ideally one day we’ll have more funding in general for sexual and reproductive health in Nova Scotia and the Maritimes,” Pink says. “My hope is we will somehow receive more funding down the road and keep building a program from there.”
While the clinic is expected to help some patients, many patients say there are just too few gynecologists working in Nova Scotia.
Jim Bentley, the head of obstetrics and gynecology at the IWK, is limited by the number of medical professionals working in the field. “I have areas within the specialty where there’s work to be done,” he says.
“I think most fields of medicine would say they are challenged by the number of staff they have; there are limitations in all areas of the province. We’re challenged in gynecological care with long waits for people, be it in the Valley, Yarmouth, Sydney or be it in Halifax,” Doctor Bentley says.
Of the 2,500 or so doctors practising in Nova Scotia, 76 of them are registered as OBGYNs with the Nova Scotia College of Physicians and Surgeons, but they’re not all working full time.
The province has roles for the equivalent of 58.4 full-time OBGYNs across the health authority and IWK. Often these full-time hours are split among multiple doctors who work in more than one facility.
Nova Scotia’s medical school, Dalhousie University, had five doctors graduate from obstetrics and gynecology in June 2021, and will have another seven graduate from the speciality in June 2022. The province hopes locally trained physicians will stick around to practice, although it’s not guaranteed.

Health minister Michelle Thompson acknowledged the concern around the number of OBGYNs when talking with reporters after a November cabinet meeting. “We have been in conversation with OBGYNs from other areas, people in their residencies, there’s a number of areas we’re recruiting specifically to,” Thompson said.
In February, when asked if the province is willing to hire additional OBGYNs, she did not directly answer. “Obstetrics and gynecology services are important to Nova Scotia women and families,” she said in an email.
When asked what’s being done to recruit specifically to the OBGYN specialty, Kevin Orrell, the doctor who’s deputy minister and CEO of Nova Scotia’s office of doctor recruitment and retention, said by email that “obstetrics and gynecology are critical parts of the healthcare system, and we recognize how important it is to recruit as many of these important specialists as Nova Scotia needs.”
The province successfully recruited four doctors to the specialty in 2019-2020, seven doctors in 2020-2021, and five OBGYNs as of Jan 31 in 2021-2022.
The number of available gynecologists varies by health zone, with most (27) working in Halifax at the IWK and the equivalent of 30.8 full-time OBGYN roles in the Central zone. The Western zone has 11 full-time equivalent OBGYNs, the Eastern zone has eight, and the Northern zone has the equivalent of 8.6 full-time OBGYNs.
Other glitches to accessing care
The long wait times are just one frustrating part of trying to get gynecological care. Since McTavish’s 2015 endometriosis diagnosis, she’s had an “extensive history of referrals being forgotten about or not put through,” which have caused major delays in treatment.
Her second endometriosis surgery in late 2021 almost didn’t happen when her pre-op paperwork went missing. After being assured by the IWK it had been sent to her address, she posted in a local endometriosis Facebook group to ask if anyone else had paperwork delays. A Cape Breton woman in the group let her know she had received McTavish’s paperwork. This woman received her own laparoscopy pre-op paperwork alongside the paperwork of two others who were set to have the same surgery: McTavish and a third woman.
“This paperwork had confidential information on it and I only found out about this breach of privacy when I posted in a local Facebook group,” McTavish says. The mistaken recipient quickly sent the paperwork to McTavish and her surgery went ahead.
“I’m so lucky the girl who received mine reached out,” she says. McTavish and the Cape Breton woman attempted to track down the third patient, but with no luck.
With and without primary care
For Karly McCurdy, a 30-year-old woman from Middle Sackville with endometriosis, the biggest shift in her access to gynecological care came when she was paired with a family doctor in 2018. Before that, she had spent nearly three years seeking help for pain and ovarian cysts at walk-in clinics without answers.
“It’s really difficult to get a referral or get the ball rolling when you’re seeing doctors [at walk-ins] who are so overworked. They just don’t have time to dig into those issues with you, so that took a lot of time,” McCurdy says. Nearly 13 percent of those who responded to The Coast’s survey don’t have access to primary care.

She says things started progressing thanks to her “proactive” family doctor, who took time to assess her and refer her to a specialist. It took one year before she was connected with the OBGYN, and then another year before she was scheduled for a laparoscopy which diagnosed her endometriosis in late 2020.
The prolonged experience of self-advocating at walk-ins and waiting for additional care can be isolating. “I’ve been left feeling like I’m on my own island, or pushed to the side,” McCurdy says.
“Care understandably is prioritized by severity and urgency, but because endometriosis is a misunderstood disease the true grasp on how painful it can be at times isn’t always taken into consideration.”
Political push
Maggie Archibald, a 27-year-old woman from Bedford, has been waiting since July 2021 for an OBGYN referral. She suffers from abnormal periods and significant pain. Her family doctor suspects endometriosis, but she hasn’t been able to get a diagnosis. She has been referred for gynecological care three times since the summer (one fell through when the doctor went on parental leave without coverage) and now she’s waiting to be seen by a gynecologist at the IWK.

“It’s certainly frustrating, it shouldn’t be so complicated to see someone who’s an expert in women’s health,” Archibald says.
“Nova Scotians are struggling with their health, particularly women’s health. I don’t think there is much of an emphasis on women’s health these days.”
Archibald has written to premier Tim Houston, health minister Thompson and her MLA Kelly Regan to express her concerns—as has at least one other survey respondent. Advocacy groups like Endo Act Canada launched a letter writing campaign in late January aimed at elected officials to push for improved access to gynecological health.
One political candidate even made it a platform. Vaginal health was the focal point of Progressive Conservative candidate Sheri Morgan’s summer campaign. Though she did not win the Halifax Citadel-Sable Island seat, Morgan became one of Nova Scotia’s best-known candidates with her eye-catching #VaginalHealth campaign signs—which feature Morgan making the shape of a V with her first and middle finger. The retired business owner ran for the PCs to support Tim Houston’s plans for a health care overhaul, she said. She wanted to run in order to draw attention to “the lack of resources in our health care system for women’s health, with a focus on vaginal and pelvic floor conditions.” Morgan was inspired by her best friend Deanne Reeve, who died from cervical cancer in 2020.
Cautious optimism
These days, McTavish, now more than three months out from laparoscopic incision surgery, is feeling cautiously optimistic. She’s currently without pain from endometriosis for the first time in many years. After two semesters off of university to manage pain and surgery recovery, McTavish is enrolled at Guelph University to go back to school this spring.
The surgery she had is not a cure, but the recurrence rate is lower than other procedures or treatments she’d tried. “I’m feeling really hopeful I’ll have a longer stretch before my symptoms return,” she says.
Coupled with a feeling of hope is lingering exhaustion, from self-advocating and navigating a challenging health structure for nearly a decade while in pain. Nova Scotia’s health system is just not built for patients like her, McTavish says.
“People dealing with gynecological issues, we’re not taken seriously by some medical professionals, we’re not taken seriously by funding. The medical system just isn’t structured to help people like us.
“I hope that the people involved in making decisions see this and realize we’re worth their time.”
To come: Next we focus on how the crisis in gynecological care affects people who want to have a baby. Subscribe to The Coast Daily newsletter to make sure you get the story in your inbox when it’s out.
Correction: The article has been corrected to reflect that Ariel McTavish studies at Guelph University, not Dalhousie.
Related Stories

The COVID vaccine side effects Nova Scotia doesn’t acknowledge

“Get over it, menstruation is normal” says Halifax councillor Lisa Blackburn

Moon Babes aims to create space for women to talk food and menstrual health

Nova Scotia’s primary care waitlist is growing (again). And the province is falling behind in its reporting.
This article appears in Feb 1-28, 2022.
I first started seeking treatment for menstrual pain at the age of 15. The only treatment I was ever offered was hormonal birth control. My body reacted horribly to all 12 brands I tried. My doctor would not refer me to any sort of specialist. I asked well over 10 times for a referral and was refused each time. She stated that there was nothing else an obgyn could offer in terms of treatment. The final time I spoke to my doctor after having an IUD inserted (a notoriously painful procedure) in yet another attempt to alleviate some painful symptoms, she said that I just have a low pain tolerance so there is nothing that can be done. This is not the only instance that I have heard of personally. Most women in my life have had an experience similar to this. It is defeating, dismissed and leaves you feeling like your constant pain is just a cost associated with being born with a uterus.
How many women in Nova Scotia are needlessly suffering due to systemic failure of the health care system? How many women have been traumatized and injured by obgyn procedures such as the endometrial biopsy? Are women and their families aware that pain relief like sedation, and pain management planning are only discussed and provided at the discretion of the Doctor; meaning that government policy does not require women to be offered or informed about pain management medication options before gynaecological procedures such as endometrial biopsies.
Why are doctors, nurses and bureaucrats telling women that procedures such as endometrial biopsies are like severe cramping and temporary discomfort when it isnt true? Research shows when no medication is provided that a disconcertingly high number of women testify experiencing intense, prolonged and excruciating pain from endometrial biopsies.
Politicians and medical professionals take an oath and are morally and ethically obligated to serve their constituents and patients.
If the provincial and federal governments dont have the money to provide health care to women then there needs to be public discourse on the issue and Canadians need to decide do they want free health care which is at half mast or a two tiered system that offers both private and public options.
If in doubt try out the endometrial biopsy without any pain management and report back your findings. Turning a blind eye only hurts everyone because the more we neglect obstetrics and gynaecological medicine the more we hurt our mothers, sisters, daughters, aunts, granddaughters, life partners and friends.
A broken health care is no health care.